
 Bruce Bassi
Bruce Bassi#FuturePsychiatryPodcast discusses novel technology and new ideas in the field of mental health. New episodes are released every Monday on YouTube, Apple Podcasts, etc.
Summary
We spoke to Tyler Beauchamp, a fourth year medical student at the Medical College of Georgia, about his book Freeze Frame. Freeze Frame explores the mental health of a teenager who slips in and out of reality during his PTSD episodes. We used this book to explore topics of hallucinations, anxiety, social isolation, as they relate to adolescent and student mental health. We also discussed very important topics of medical student mental health as it relates to residency applications, self-disclosure, judgement of others, fear of seeking treatment, and stigma.
Chapters / Key Moments
00:00 Preview
04:05 Mental Illness & Misperceptions of Reality
11:09 Being an author and it changing your identity
13:29 Hobbies not worthy of public disclosure
16:40 Isolation and impact on mental health
20:34 Paradox of receiving care and becoming a better clinician
30:20 Self-disclosure in medicine and medical school
37:56 Contextual errors
39:57 Stigma of mental illness in medical school
45:34 Why disclosure should be praised and celebrated
55:13 Insights into social media addiction
01:07:16 New future treatments in child & adolescent psych
01:12:49 Perspective changes on the book
Transcript
Tyler Beauchamp: The more he’s including them and the more that he’s talking and being vulnerable about himself, the more that he’s engaging in therapy, that he’s not having these episodes. And it’s when, you know, out of fear that his family puts them in isolation, that they’re actually doing more harm to him. And that’s when he realizes the necessary steps he has to take. And so that’s what I hope for people to be more on honest about in med school, at least for the mental health aspect, is that these things may occur and they may either arise before or during or even after med school. But as long as you are taking your effort, your tangible impact that you can make to not be the limiting factor yourself in your health, then that should just be flat out encouraged. That should just be supported and praised.
Bruce Bassi: Hello and welcome to the Future Psychiatry podcast, where we explore novel technology and new innovations in mental health. I’m your host, Dr. Bassi, an addiction physician and biomedical engineer. If you are joining for the first time, I would greatly appreciate if you subscribe and share it with your friend network on social media. Additional resources, a full transcript and group discussion form can be found on our website telepsychhealth.com, then click podcast in the top right corner. Thank you so much for joining us and I hope you enjoy the discussion today. So today we have Tyler Beauchamp, a fourth year medical student at Medical College of Georgia and author of the book Freeze Frame, a coming of age fictional novel that also explores the psychological mindset of teenage life. Obviously, med students in your generation are the future of psychiatry and future of treatment for patients. So I wanted to reach out to you to talk about your book, your background, med school stigma related to psychiatry, all that good stuff. So welcome to the show.
Beauchamp: Thank you so much for having me. I’m happy to be here.
Bassi: So I know that COVID really spurred on your interest in writing a book. And also you mentioned that you’ve just always been interested in writing. You felt like you were going to write a book at some point, give us a little bit of background about how that came about and what that process was like, balancing medical school with writing of a book.
Beauchamp: It was a lot, for sure. But it’s funny, back then when I was growing up, I thought I was just going to do writing, and when I came across medicine, I was having to decide, am I going to do one or the other? So I put writing aside for a little bit to just focus on getting into med school. And it was funny that once I got into med school, with the added stress compared to college, I needed more outlets, so I found myself writing more than I had in my entire life in med school. Just either a short story here or a poem here. And nothing was more stressful, of course, for all of us when the pandemic began. And so we were immediately shifted into online virtual med school, at least for us. And I was just ending my first year, wrapping into second year. And so you’re not really in the wards yet, so you’re really just online lectures and studying from home. And we weren’t really allowed in the hospital for the most part to help out and volunteer because they were trying to keep numbers down. And so you had a lot of time just to yourself. And for me, I was literally living in this room with no windows and it had this malfunctioning door and it felt like a prison cell. And I started having these ideas about kind of jumping in and out of daydreams because I was just wanting to get out. I felt so stressed and boxed in and so I started writing this story, not even intending to publish. It was just an escape for me at first. It was just a nice thing to do at the end of the day, something different than studying. And the more I went with it and the story of this kid who was struggling in high school in his own box, as if he was in my room, but just walking around the halls surrounded by people, but feeling alone. It just felt very moving and I could relate to at the time. The more I went along with it, the more I thought this might be a story that some kids could read and relate to as well.
Mental Illness & Misperceptions of Reality
Bassi: Nice. You mentioned going in and out of reality because of being in this enclosed environment, a room that didn’t have any windows, kind of feeling locked in. And that reminded me of a syndrome called Charles Bonnet syndrome, wherein if you have some sort of sensory deficit like in your vision or in your hearing, your brain actually starts to fill in those gaps with hallucinations. And I feel like we’re all just really one breakdown away from having hallucinations. People kind of come to me without schizophrenia, having had the experience of hallucination. And it’s very, very scary. You don’t know what’s going on. But in fact, it’s not uncommon for people to withdraw from substances or be sleep deprived or be in and out of sleep or have some variant of Charles Bonnet where there’s not enough sensory input and actually experience hallucination. And I think that’s a fascinating concept to explore in a book with a mental health backdrop because a lot of mental illness does come down to a distortion of our version of reality, really. And like depression, for example, you’re probably thinking lower of yourself or thinking lower of the world around you in a way that’s not really representative of the true reality. You’re hyper focused on these certain cues. Same with anxiety. You might be hyper focused on more internal cues versus external cues or maybe some external cues that you really don’t need to be focused on, or you might be misperceiving an external cue. So I think that there’s a lot of really good teaching points when talking about these things in the book. Do you have any thoughts on that?
Beauchamp: No, absolutely. So people ask, what was the main character’s official diagnosis? And I guess for the purpose of the story, I tried to keep it more of like an atypical PTSD. I was trying not to make it one draft I had, it was not he was suffering from multiple disorders, and it was a full swing of diagnoses. And I realized the more I did that, the less realistic I could make him still be in high school functioning. Because at that point, someone at that level would need more serious help than just an outpatient child psychiatrist. So it was weird battling the realities of psychiatric medicine with also an engaging story, because you have to think about it from both perspectives and how realistic do I keep it in a story that is inherently unrealistic at times? Because he is going in and out of reality and you’re seeing it from his perspective. So there’s some tailoring down on that. Because if I wanted to reach out to kids that could relate to this, for the most part, the kids that would be seeing it would be kids who are functioning to some level in high school.
Bassi: Right. Yeah, exactly. Your audience is YA, young adults. Right. So understanding that you’re talking to a teenager, not necessarily a colleague, do you mention PTSD in the book?
Beauchamp: I do a little bit.
Bassi: Did you debate doing that or no?
Beauchamp: For a second I didn’t. I think in the second draft of the book, I took out everything from that. But then there are a few chapters where the story goes on and it’s interspaced with meetings with his psychiatrist and without any discussion of official diagnosis with him. It seemed a little disingenuous that they would meet that many times and not talk about, at least theorize what’s going on, because the main character even questions like, what’s happening to me, my normal. And so I tried to keep it vague because I didn’t want to focus on the diagnosis, I wanted to focus on his journey. But I eventually included in some discussions about that. Just because you couldn’t have that many meetings and not talk about that at some point.
Bassi: Do you feel like to a reader who has had childhood trauma, this somewhat I wouldn’t say normalizes, but validates their experience?
Beauchamp: Absolutely. That’s been one of the most rewarding experiences from releasing this book, is having I’ve had a few people come out to me after reading it. Some kids I’ve been doing some tours at schools and talking with middle schoolers and high schoolers, and a few of them have come up and said, no, I didn’t have what happened to him happen. But I have had the feelings that he’s had and the isolation from those feelings and the way that Will, the main character, responds to his events is very similar to how they say they’ve responded to theirs.
Being an author and it changing your identity
Bassi: Wow. Nice. I think that’s, like a motivating factor for why many of us go into medicine to see a positive impact. And with a book, I think that’s really cool. I’m a little jealous in a way that seeing you on your journey, that’s pretty awesome. To have this tangible impact on so many people around the country and have them tell you how it’s impacted them.
Beauchamp: It’s been really wonderful. I just got back from Augusta. I was doing a Barnes and Noble because now that I’m in Barnes and Noble, which is really cool to say. But I was doing a fundraiser with the Children’s Hospital because my home base is out of Augusta and so all the proceeds were going back to the Children’s Hospital. So we had a big turnout at the store and I had a mother come up to me and ask if she wanted to know what the trauma was about because it talks about trauma in the back story. And she wanted to get the book for her daughter. But her daughter was interested in film and art and she said, “Can I ask what the trauma is about?” Because my daughter has recently gone through something. I want to know if it’s something similar. And I go, well, it deals with a death of a family member. And she started crying because she said that her daughter and her lost her husband, the daughter’s father. And I said, well, if you wanted to read it first or if you wanted me to highlight certain chapters to leave out, if she doesn’t want to experience that, I can totally do that right now for you. And she goes, no, I think this is something we could read together because she’s been wanting to talk about this experience and the people around her are kind of hesitating about how can we talk about your dad? Can we not? Like, how do we treat you? And she just wants to talk. And so I gave her my contact and said, Let me know how it goes. And if she wants to write as well if there’s anything I can do to help out with writing in the future, let me know. So that was a really cool experience I wasn’t expecting to have at this middle of Barnes Noble.
Bassi: Yeah, that’s really moving. That’s really awesome. And really nice of you too, to offer to do that. How has the book kind of become part of your personal identity and has it changed who you see yourself as personally and professionally? Our identity is somewhat how we see ourselves and how other people see us. And I don’t know if people make certain assumptions about you based on the book itself. Now, when they meet you or not? Just kind of curious.
Beauchamp: That’s a great question. For a while, when I was writing it, I didn’t tell anyone that I was writing it, especially around my class in medicine, partially because I was worried people might think I wasn’t focusing on what I needed to be focusing on. That was some worry there. And it never got in the way of my studies and work. It was just always something I did after. And when it got closer to it and I talked about it, I think it was kind of met with that response of, oh, that’s cool that he’s doing this project, but I’m not going to take it too seriously. And then once it was actually published and people kind of had the response, oh, wait, you actually wrote it? You wrote this is real. This is a real book. It’s on Amazon. It’s going around like yeah, that’s what I was trying to say. So there’s definitely a lot more credibility to it now that you can have it in your hands. So the response has been great. And people definitely when I go and see people, that’s definitely what they want to talk about most with me right now. It’s funny because in my head, I actually finished the story almost two years ago. And so after a lot of editing and marketing and this kind of press tour then on for me, I’ve just been excited to write the next one. I’ve got these stories that I want to get out there, and every time I’m starting to work on them, I have to go back and help with this thing, which I’m so happy to do. But in terms of this, with my identity, I see myself more as I’m just really excited to do the next one. I want to get this next story out there and see how it can move people too, hopefully.
Hobbies not worthy of public disclosure
Bassi: Yeah, you brought up a lot of really good points there and a lot of ones that I can easily relate to as well. Doing a podcast, people might think that was one worry I had, too. Like, don’t you have other clinical responsibilities to do? But you mentioned this on some of your other podcasts. I think we need this balance. We need a little outlet, creative outlet especially, to kind of keep us grounded, keep us balanced, and provide better clinical care. I think it helps us know ourselves better too. And I think one thing that’s cool about writing a book is that it’s something you can talk about with residency directors because it’s a professional outcome, something that you made that looks really well polished and nice, you guys, on your podcast, I thought it was funny. One of the hosts brought up how there was an applicant who wrote down none for Hobbies. And I started laughing so much because I can kind of understand that when somebody is a med student, maybe you don’t think that some of your hobbies rise to the level of being disclosed. Maybe you work out at the gym or you go running or you listen to podcasts or you like YouTube or you just want to pass your time and relax as a student. And maybe they’re like, I don’t think any of these are worth mentioning on my application. So they just put none. Didn’t think about how that would come across. But you, on the other hand, you wrote a book and that’s like, obviously very commendable and pretty awesome.
Beauchamp: Thank you. In that podcast that we do, the Tales, Tunes and Treatments, we started that because the guy that I do it with, this is a guy that I do music with. We had done like a music video for COVID and then we write songs together and when he went off to rotations and we kind of got separated, like, how do we keep our creative outlets going together? So the podcast was like the natural next step so we could keep talking about being creative in medicine. And at first it was just going to be for us. And then we started talking with other people in our class, in the classes near us, and people started sharing their own creative outlets. They’re wondering, could we talk about this? Because it’s something I don’t have to go on a big stage and do this. I can just talk about it with YouTube. And we got students that like one was she wants to be a neurologist and in her free time she’s a painter and she paints different neurological pathologies and how you would experience them if you had it yourself. So she’ll do the same painting like ten times, but it’s differed in each painting with a different visual deformity. And it blew my mind. She’s like, oh, I’ve been doing this for years. This is something fun. And so I put it on my website and got her to talk about it. And then other people are asking her how she does that. So part of being creative for us in medicine is, yes, to keep us grounded, insane, and it keeps us alive. But also we’re kind of hoping with the way medicine is changing with providers, that it will help inspire others to approach things differently, to attack the problems that we’re currently faced with new creative avenues.
Bassi: When I decided to start a podcast, I was like, how are people going to perceive that as being maybe a little cliche? Everyone has a podcast these days, but ultimately it’s like a win win for both the host and the guest because otherwise you would have never had this conversation and also allow it to be brought to millions of people, potentially. I mean, I’m speaking for other podcasts too. Say the podcast didn’t exist. Nobody else would ever know about this person or this idea, how it came about. So these are conversations that, if I didn’t have the podcast, I would never have been like, Tyler, let’s just go talk for a little while and get to know you in the book and how it came about and how some of these ideas relate to child and adolescence, psychiatry and stigma and different perceptions of reality, et cetera. One other theme of your book talks about a lot about inclusion. I think Will Horner is his name. He has mental health struggles that parallel and coincide with how included he feels in people around him. And obviously, that fits the theme of med school when we’re trying to adapt to a new rotation, when you’re first joining med school, when you are going to residency, there’s a lot of that struggle, and I do think that does have an impact on one’s mental health. Social isolation hits the same circuitry as pain, the anterior cingulate cortex, and it feels very physical at times. And maybe we can talk a little bit about that, about how your character struggled with isolation and how it had an impact on his mental health.
Isolation and impact on mental health
Beauchamp: So I was very intentional about not only when I wanted him to be isolated, but how he perceived his own isolation. So when the story begins, he is isolated, but he prefers to be. And that’s actually when he’s nearest his worst, because he’s so afraid of anyone seeing this side of him after he had his whole world exposed at a previous school. That’s why he’s going to a new school, is to get away from that. He’s just running from the exact opposite of being isolated. And the more and more he’s brought into the fold by this new group of friends and he’s working on minor steps with his mental health therapy, the frequency and the severity of his episodes are actually gradually going down. And it’s not until there’s this kind of drastic not the climax, but kind of like secondary climax of the book, where he’s pulled away from his friends and he’s most literally isolated in his room by his family that he went from almost no episodes for, you know, four or five chapters to episode, episode, episode, back to back to back. And I remember I was speaking with an editor and an early reader at that time, and the editor talked to me about pacing and saying, like, hey, I’m reading this first. And you have this gap where he’s having none of these breaks and episodes, because to a reader, those are the exciting things. It’s the breaks from reality, what you’re experiencing, and then suddenly you have them all at once. Maybe you space those out. And then I had an early reader come in who also had some medical background and goes, this is beautiful, because it’s so subtle that he’s not even realizing himself that this is his fix. That the more he’s including them and the more that he’s talking and being vulnerable about himself, the more that he’s engaging in therapy, that he’s not having these episodes. And it’s when out of fear that his family puts them in isolation, that they’re actually doing more harm to him. And that’s when he realizes the necessary steps he has to take for the end of the story. And once I kind of explained that side of the editor, they were like, oh my gosh, I wasn’t even thinking about it that way because they hadn’t gotten to the end of the book yet. And you know, I was also very intentional with the end of the story that Will is in no way healed at the end of the book. It’s not necessarily a sad ending. It’s just a realistic that he’s found. He’s found the right road he needs to go on. And it’s up to you to really decide if he’s really going to go down that road. And I try to make it clear that he feels confident that he will. But the message of it is to take control of your therapy and to have the courage to be vulnerable with those around you in that, to be more open about that. That’s definitely something that we’ve struggled with as students in that school. There are a lot of mental health stigmas within medical education and kind of keeping things pushed down and just fighting through. There’s a lot of worry about seeming weak at times because it’s weird. If you are going to be the provider of someone’s health and if you are going through something yourself, then some people think, well, then I’m not worthy of being able to provide, or I’m not capable of being able to provide. Even though it’s the opposite, you actually can maybe understand what the patient is going through on a different level, a unique level. Now, you still need to take care of yourself. You still need to go through the right avenues. But I think we’re hopefully getting closer to a state in medical education where people are understanding that more. I’m hopeful about that.
Bassi: Yeah, really well said. A lot of good points you made there. Thanks for your insight on isolation, especially with patients. There is this paradox where all of our psychiatric illnesses, they’re kind of pro isolatory. They move you towards this isolated state. Or I heard this concept where evolutionarily, depression, maybe had some sort of benefit by getting you to start to problem solve withdrawal from other areas that maybe were not that important in your life and try to introspect and figure out what you need to do to fix some problem. And maybe at some level that’s now maladaptive because it’s pulling you away from people, but what you need is the exact opposite, but nobody wants to do that. So it’s a cool idea and one that I’m thankful that you kind of illustrate in your book, because obviously people need that reinforced constantly. When you are in this depressive state, you’re you’re just seeing reality a little bit different than you typically do. Kind of reminds me of how suicide survivors they often say that there’s this I don’t know if you’re familiar, there’s a there’s a club of people who survived the Golden Gate Bridge jump. There’s like less than 0.1% of people. They say right when they release their fingertips from the railing, they have this intense zest for life again and intense regret for what they’ve just done, praying to God that they’ll survive the fall and thinking that they now see everything as kind of insignificant right before their eyes. There’s actually a guy, I think his name is Kevin. I can’t remember his last name, but he is a motivational speaker now because he survived the Golden Gate Bridge fall. And he now talks about this. And it just reminds me and it kind of relates to the theme of your book, this misperception of reality and how it relates to depression and anxiety. People just regret it after they’ve started the ball, moving the ball towards suicide. Thankfully, some people fail in their attempt towards suicide and they have another chance to kind of reevaluate themselves in their life and start to live a good life again. I like how we kind of piece together this altered sense of reality with isolation now.
Beauchamp: Yeah, really, it’s interesting for sure.
Paradox of receiving care and becoming a better clinician
Bassi: You mentioned stigma within medical school community and that’s one topic that I really want to talk about with you. And we’ve kind of uncovered a few themes here. One, if you cultivate an area outside of medicine, people are going to be kind of judging you secretly.
Beauchamp: Isn’t that so odd? I just remember applying to college and feeling like if I wasn’t doing a million different things, then I’d be behind and then applying to med school and feeling the same thing. Even though you’re narrowing your life at this point, you’re going to a professional school, you’re not going to college. And I felt like, okay, so once I got in, I was like, well, maybe I can take a little bit of a breath and that I can just do what I love now I don’t have to worry about kind of meeting all these certain bars and standards. It’s not isolated to my medical education. It’s definitely when I speak to friends across medical schools, the second you do all these things to show how well versed and well rounded you are to get in, but then the second you’re in, you’re very much encouraged to shut all of that other stuff off and completely focus on the one thing. And then they wonder why there’s higher burnout and they wonder when we get through it, why people can become easily jaded. Part of the reason you encourage someone to be well around it in the first place is to be more human one thing, but also just you can have new experiences that you can relate to others. So it’s an odd double standard for sure. And the good news is, at least in my school from when I started and now I’m entering my last year, it almost feels like a completely different environment when I speak to the incoming M ones because we have done a lot to at least recognize some of this. Not like hypocrisy, but double standard nature that medical schools are there to get you into residency, and they’re just as afraid about, like, under preparing you for residencies and what residencies are looking for. And if something’s always been done the way that it’s always been done, and then there’s massive changes to the system and no one really knows what change is going to be better to get you there. They’re going to stick with the flow. So a big thing, this might be integration but a big change for sure. In my time was two things. One step, one for those that don’t know listening, the first of your major board exams, that used to be the standard for I guess what residencies would look for, for you. It was a very stressful score and test that was made pass fail during my time and then also with the pandemic occurring during my time as well. A lot of opportunities that students normally had to work in certain levels or research, a lot of stuff was just cut off. So a lot of the benchmarks that students had to set themselves up for a job and interviews those they’re gone. The question became what do you do now? What do you do to compare like students? And for the most part it seemed like people were just grasping us draws and we won’t know until the data shows us, we won’t know until this next class and the class after have gone through because we’re in a whole new world when it comes to that. And so what I hope and when I am starting to see a little bit from hearing about the interviews that the class above me are looking for during the interviews, they’re asking a lot of things that are extracurricular because that’s something now that you can use as a benchmark for other comparisons. You know, my co host for the podcast, he’s going into radiology and he does a lot of research and he’s done well in the scores and in almost every interview he’s had, they have not asked about the research or scores. They’ve asked what’s your podcast about?
Bassi: They want to know him, who he is.
Beauchamp: Yes, which is great because they’re looking for a colleague. They’re looking for someone who can I spend eight to six with or just work the week with too. So I’m thinking we’re getting to a place now where because of all the changes that have happened, they are going to be looking for people to maintain things outside of medicine that keep them human and put a focus on who you are as a person, not. Just who you were in your scoring in med school.
Bassi: Yeah, totally. I think residencies by definition, they need to judge their candidates and whether or not they want them. So if you eliminate scoring, they’re going to find another way to judge them. What was the consensus like, the feeling when they made step one pass fail? Was that a welcomed a relief? Or were people like, now how are they going to judge us now? What do we have to do instead? Are there strings attached to this?
Beauchamp: Oh, you know, us medical students, we were stressed beyond belief. I’ll be honest, I wasn’t too stressed because for me, I kind of heard it and just like, well, there’s nothing I can really do about it at this point. But there were a lot of questions that seemed unanswered by everyone. We would go to advising, we’d go to up high and ask, so what do we do now? And they don’t have the answers either, because it’s a whole new world. So at least in my class, there were only a few people that had already started fully preparing for a step score. And then they were, of course, a little frustrated because that work. They could have been doing something else. I think whenever you make a change at that level and you’ve sacrificed so much to get to this point in your career for med school, a change like that fundamental, it’s just going to cause stress. And I felt it’s put a lot more pressure on step two. Now it’s kind of– you have one board score and one shot. This is it, one take. And so at least I don’t take mine until March. But the people in the class above me, I’ve talked to them about it, and it was a very difficult time for people to get through, for sure.
Self-disclosure in medicine and medical school
Bassi: We can talk a little bit about self disclosure. I always find this topic to be something that I grapple with a lot, both when I was a med student to figure out how much to self disclose to residency programs as a doctor, to figure out how much to self disclose to patients. And I think there’s a movement right now from my experiences in using social media. People want raw, down to earth individuals who they can relate to and understand, who come across well, and the more polished and professional you are, it’s almost like those videos don’t turn out well, and they don’t get as much engagement. And I think there’s this movement to kind of to know people in their most authentic self. Right. And I recently wrote an interview piece for The Mighty, and they were asking one of the main questions was like, what is the misperception of psychiatrists? And I wrote that we’re robotic, that we have no emotions. And I think that stems from the fact that we’re trained to not self-disclose so that people can do their own self analysis in kind of like this very sterile environment with no outside impact. I think self-disclosure is a very fine line because it can easily be taken the wrong way. Like it was too much poorly timed, self-centered. I could think of numerous ways people can criticize something I disclose because there’s this power differential. They think you’re a doctor, they think you got it together. They think you’re wealthy, they think that you have everything you want. They think you’re on the ivory tower. There’s all these stereotypes. And so doctors and med students probably often feel it’s a liability to self disclose, especially doing a music video. Or when I was a med student, our class did a music video, but I was reluctant to be in it because I didn’t know what way the residency programs would be judging me. At the time, a lot of other med students were changing their names, like on Facebook. They didn’t want to be found anywhere on social media. They didn’t want to have any internet presence digital footprint at all. It was just this fear of how are people going to think of me and how are they going to judge me in a negative way. Everything I disclose is a liability. I want it to be polished to the utmost extent on my application, my ERAS application, and that’s it. So it’s nice kind of hearing your perspective because I can’t believe it eight years out of med school now and kind of seeing how I think things are changing. Slowly but surely they’re changing. What are your thoughts on all that?
Beauchamp: I have so many thoughts, two quick things on that that really are close to my heart. So I told you this part of I had to take a brief leave from med school because I had a few medical issues come up. And it’s so funny, I was wondering, where do I put that in my ERAS application? Like, how do I talk about this? And I actually got a lot of advice from advisors, current residents, people at different programs, just like that I knew of from friends. And it was actually pretty split on whether or not to actually say I had to take medical leave. Yeah, and I was shocked by that. And they said, yeah, make sure you can get research done in this time and do your medical leave during that time as well. But just say, like, you took that time for research. And I was like, why would I not just be honest. If anyone would understand that I had a medical issue come up, it would be a residency. And a lot of them were split on that issue, actually. Not that it’s a weakness, but it could be seen as will the issue come up again during residency to take you time away from that? Is it not something that you can take care of when you have things arise in your life? Can you not take care of them with your work going on.
Bassi: Yeah, it shouldn’t be a weakness, but it’s certainly not a strength to disclose it’s the way it’s perceived and felt.
Beauchamp: Right. Correct. I was terrified. I was like, oh, my gosh, I’m going to doctors appointments and getting scans and stuff, and I’m doing my part as a patient. And the whole time I’m wondering, oh, is this going to keep me from getting a job after all this? And even when I wrote the book, I was told by a few people to write it under an alias. Interesting. Because they were like, what if a residency reads this and they don’t like the message that you’re saying? Or maybe they just disapprove of the fact that you did that during medical school. Maybe they’ll see it as the opposite. And fortunately for me, it has not been that case. It’s been met with a lot of support in the medical community, which is great, but I did have this fear in the week when I was getting ready to publish. I was filling out all the paperwork and the tax forms and stuff, like, who is the author? And I went back and forth. I was like, I don’t know. I’m being told so many things in so many different directions. And I basically I had to make a similar decision at the same time with the book and medical what to do. And I just came to the conclusion that if a residency is not going to want me because I had to take a medical leave or a residency is not going to want me because I wrote a book that is not a place that I want to work at for three or five years. I want to work at somewhere where they encourage you to take care of yourself and they encourage you to pursue outlets that hopefully help others, too. It’s like you said, the authenticity and being genuine, it’s something that I could never tell down the line when I’m a physician and I’ll have med students and people asking me questions the way that I’m sure you get all the time, I could never tell a student not to be honest about a medical problem. I could never tell a student to not be proud of some publication that they did because they should be. So because I’m thinking about that long term, it would just be wrong for me to do the opposite now.
Bassi: Yeah, that’s so interesting. I think maybe, like you said, it speaks to the person, other person. Like, if they’re saying don’t disclose it, it could be seen negatively. I think that probably speaks to the other person’s experiences with other individuals who have had medical problems. Maybe they, like, saw them as a nuisance or something like that. Now they’re kind of passing that judgment on subsequent student, ie. Yourself.
Beauchamp: And I think it also is specialty dependent, unfortunately. I think a lot of specialties will treat it differently. Yeah, I was going to say that, too. Yeah. So a few of them were at, I guess, viewed as more competitive, specialties. So I can see the fear being more common in those where the margin for error in people’s eyes is a lot slimmer.
Bassi: One of the first comments on the mighty post that I wrote was, “I wish doctors would self disclose more, but I get your point.”
Beauchamp: Yeah.
Contextual Errors
Bassi: So there is this appetite for doctors who are a little bit more relatable, I think. And I think maybe that should be part of the focus in med school. Like trying to there’s this concept, maybe it’s not new, but I’ve kind of heard of it described this way, called contextual errors, and how to understand how treatments can have contextual errors associated with them, where you make a recommendation, yet the person doesn’t have the resources or memory to actually enact that treatment recommendation. So on the medical record, if you were doing retrospective study of the record, it looks like you did a really good job. Yet that patient actually isn’t improving, and they haven’t gotten any of the treatment because they don’t have access to it, or it’s too expensive or it’s out of their area that they can travel to, et cetera. And it kind of relates to what we’re talking about because I think patients, from the feedback I’ve gotten, the more relatable you are, the more attractive that actually is to that.
Beauchamp: Absolutely. For one, establishing a connection of any kind. For a lot of cases, you walk into a room and you’ve never met someone and you’ve got 15 to 30 seconds to establish a close bond.
Bassi: Over and over and over again.
Beauchamp: And over again. And so what better way of bonding with another person human is just having a shared experience, having something that they can relate to. If they know that their doctor understands a level of them on a personal level, or even just on an empathetic level, they don’t have to go through the same experience, but at least they know that their doctor understands them. One, they’re going to be more forthright with information, with their care. They’re going to take more ownership of their own therapy, but also just for returning for continuity. That’s a big problem that we see that patients can establish and get going for one, two, three visits, but maybe fall off. But the more that they feel that they’re working with their physician, not their physician, is just treating at problems, the more likely they are to keep coming. So that’s a huge benefit.
Stigma of mental illness in medical school
Bassi: Yeah. I want to wrap up the idea of stigma of mental illness within medical school. I think it’s still a problem. When I was a resident, I remember some medical students voicing their experience about how they weren’t really supported in their leave from medical school for mental illness. And it’s almost like you said, there are good leave of absences, and there’s kind of bad leave of absences where people will be like, what did you do? Is that going to come up again? Do you have control over that? What was the entirety of this circumstance? So I can judge you better. It’s impossible for me to compare my experience to yours, but how supportive do you think self-disclosure is of mental illness within your class? Perhaps?
Beauchamp: So I’m very fortunate with the class that I was in. We were very supportive with each other in that it was interesting that we had a little bit of experience together in person before COVID So we had like, nine months together and then the pandemic hit and then everyone is isolated from each other, but we at least knew of each other. You know, the class below us, they came into med school and, you know, some of them went two years without actually meeting other people in the class until rotations, until wards. Anna, is this wild? So those first eight months, I think people were afraid to be open about one. You’re just also meeting people for the first time. So you’re not going to just tell everybody that you just meet, hey, here’s all of my problems and baggage and everything. But once we were in the height of the pandemic and it had been a few months of isolation for everybody, that’s when people really started opening up to each other. At first it was just independent. Like, I get a call from somebody, hey, I really need a vent about what’s going on with my life. And then you’d go back and forth and then that transition more to a group me setting where people would establish zoom calls. Let’s kind of talk about these issues as a group. And then that went to more of a class to administration, like, hey, this is what we’re all feeling right now. What things can we do to address these? So it built for there. So I was very honored to be a part of a class that supported those kind of things. And I think for the most part the school does too. And I do think there’s still some fear with, well, we do support these things, but do residencies. So for me, when I had my medical leave come up, it was a combination. I had a mental health problem I was working on with my psychiatrist and I had a GI problem that was going on and they were both pretty severe. And I was going back and forth across clinics and getting referrals to other cities for some of the stuff. And it’s like you said, you kind of have to pick what’s going to be seen as the better one to view as. And so GI as one of the systems I was going through was a more explainable and understandable problem to have for residencies is what the thought was, and it’s not lying. I had a pretty serious GI problem come up. But it’s unfortunate that I had to meet with that fear. I couldn’t talk about a multi-system problem that was happening. And I’ve had a lot of thought about when I interview and talk with programs and if they ask about that time, what will I say? Like, will I talk about the others? And I’ll be honest, I go back and forth out of fear myself. But I think I’ll probably talk about both. It’s just because at this point, like we said, I don’t want to go to a program where that’s not okay to I guess we talk about this a lot with the mental health problems that are pervasive not just in the medical community, but in our world right now, they can be more easily seen as weakness. That’s the stigma compared to other things. Right. And I think it’s because when those problems occur, people outside of that don’t get to see the tangible improvements that patients progress through. But I have tangible steps I can talk about that I took with my psychiatrist at the time. I have tangible steps, and they were not easy in the slightest. The process I was working through with my GI docs and the surgeons and the processes I was working with my psychiatrist. I knew that if I go through each step as hard as I can and as full as I can, I can talk about it from the sense that, yes, these things happen to me. But I didn’t let those hold me back to the best of my ability. That’s what I hope for people to be more honest about in med school, at least for the mental health aspect, is that these things may occur and they may either arise before or during or even after med school. But as long as you are taking your effort, your tangible impact that you can make to not be the limiting factor yourself in your health, then that should just be flat out encouraged. That should just be supported and praised.
Why disclosure should be praised and celebrated
Bassi: I was exactly going to say that because you know how we were talking earlier about how our mental illness can kind of pull us in one direction, but it’s actually not what we need. We actually need to go the other direction and lean in. Yeah. Most residents at some level can struggle with depression, anxiety at some point in residency. And wouldn’t you actually want a resident who is open about understanding what that is and seeking treatment for it, rather than one who’s the opposite? Therefore, wouldn’t you kind of praise and encourage people to have that open conversation as an applicant so that the program director is actually no, this person? Well, yes, they may have struggled with mental illness, but so have most people, and they actually recognize it. I had struggled with anxiety throughout medical school. I didn’t actually see a treatment provider until my intern year, and afterwards I was like, what took me so long? What was I waiting for? And I’m somebody who is a mental health professional. I’m plugged into mental health establishment. I know how to seek treatment better than a typical person, I would say. But yet it took me four years to actually seek treatment for it. And I probably couldn’t safely say I waited for it to get more severe than if I had recognized the importance of treatment earlier while I was in med school, because therefore, it was just kind of being untreated and I was just kind of struggling with the symptoms and the impact it was having on me rather than actually going forth and getting treatment.
Beauchamp: And for you, it might be a combination of the two. Was it more fear of what people would perceive you as, like, the higher professionals in the field, or was it more you may struggle with anxiety, but that’s just natural. With med school, that’s just normal. Everyone does. So you’re no different than the next person next door.
Bassi: I would say it was a combination of I wouldn’t say fear, although probably if I got treatment, it was fear. I would say it was more of an ignorance of what impact treatment could have had and also the intermittence of symptoms, they weren’t constant. So I was like, okay, maybe I can get through this. And then we just kind of peek back up at the most inopportune times. And so that inconsistency was very confusing and I think also makes people not and now that I think of it, I did go to student health services, but of all things, they gave they just gave Xanax.
Beauchamp: I was going to say, they probably just gave xanax.
Bassi: So like you said, it should be praised and celebrated, but heart easier said than done, perhaps.
Beauchamp: Yeah, maybe the conversation will change that. If someone went through a mental health struggle and either went through it not to say that it’s over, or at least has found tangible treatments for themselves that would be more of an asset for the team when their residents, unfortunately, may inevitably face some form of mental health struggle in their time of the three to eight years that they’re together. That’s at least how I would view it if I was running a residency program. But maybe one day.
Insights into social media addiction
Bassi: Yeah, one day we will eventually have the ability to have an impact on these things that we’re talking about. Maybe we can kind of flesh out the idea of the book and how it relates to you and your endeavors kind of in the future. Pediatrics, I think, kind of like my experience, a lot of mental illness comes through primary care first to begin with, and 12% of children have ADHD, and I think it’s about 10% of kids have anxiety. So you’re going to be seeing a lot of mental illness as a Peds doctor if you do outpatient and don’t subspecialize. But I think that your ability to write this book and explore these mental health topics will make you a very strong Peds physician.
Beauchamp: I sure hope so. Something I noticed, and maybe this was because at least I didn’t really grow up with video games. I grew up heavy with film as it was influenced by the book. My my dad works in film and sound, but we we always approach film as more like analytical. We’d sit as a family and we’d watch films and we’d pause and talk about character development and shots and stuff. So it’s very atypical, for sure. But screens weren’t a big part of my upbringing and of course, that’s the exact opposite. Today you cannot find in pediatrics, you cannot have a kid come in with family and someone in the room, not on a screen, whether it’s one of the parents or the kid. And unfortunately, it’s very weird also for me now that I’m only 25. But a lot of times I’ll have patients come in and their parents are younger than I am and I’m thinking like, oh, I’m still a pediatric patient in my head. I haven’t been removed from pediatrics myself that long, but I think a lot of the parents were raised, if they’re younger than me or around my age, as screens as a solution because it’s an easy distraction. If a kid starts crying or if a kid is nervous, you give them a screen and just like, okay, we’re going to take focus off for a second rather than address the problem at hand. And with a lot of stress that parents are under and there’s no easy feat to parent a child, you look for the little wins. And unfortunately, a huge thing I see in pediatrics is people putting off solutions for temporary solutions. The antagonist of the book, they’re called the ‘Content Crew.’ And so the main kids, they’re all making a film together. It’s an art school. They’re trying to make this movie for a competition and everyone in the school puts some sort of artistic feature in for this big prize. And the main group, they’re very counterculture and they’re making a film on an actual camera using real sets and everything. When most people say they just use your phones and everything is 1 minute or less, for sure. So the content crew are these young social influencers. And it feels weird to say, well, they’re in high school. They can’t be social influencers in high school. And that is not at all true anymore. There are kids in high school with massive, massive followings. And so these main two, they’ve got one on YouTube and an Instagram and a Twitter, they kind of all combined. Someone called them like the infinity gauntlet of social influencers in high school. And basically they have to battle, how do we make a film that grabs people’s attention in high school when one, their attention span can’t go longer than a minute to five minutes. And two, they want to like these content crews’ videos and creations because if they like them, then they’ll like them back and that will help boost their own status in high school with their platforms and everything. So everything is very disingenuous from that side. And a lot of the stress around the high school and the kids development in that is that the social hierarchy of kids has completely changed. Like the kid comes into the school and he sees like jocks kind of sitting at a table, but no one really cares because they only have like 100 followers. Whereas this scrawny kid who’s got a YouTube channel with like 100,000 followers, they’re all flocking to him. And so it’s like, what? Okay, so it’s not about how fast you can run or how athletic you are and it’s not even the nerds or the nerdy ones. It’s all about social influence. The popularity has like defined metrics and with that kids are learning to not put their most genuine self forward, but rather the self that is gaining these numbers on whatever platform they use. And using that, once I realized that that was going to be like the primary antagonist protagonist dilemma, fighting between these all these avenues for little moments of what stressor does a kid in high school go with from here that arose? Or like, how do I make this scene of we’ve all had it a million times where someone puts something online and then no one likes it and how they internalize that. It felt so odd because I myself am not very big on social media, but I have all these experiences working with these kids where that’s all they they talk about and that’s how they view life. The number one do you know what the number one most wanted job was last year out of graduating seniors in high school?
Bassi: Influencer?
Beauchamp: YouTube creator, not a doctor, not lawyer, not any professional. It was number one was YouTube creator and second after that was, I think, just general social influencer. Isn’t that wild?
Bassi: But oh my gosh. What has your book kind of shed on social media? Addiction, internet addiction, phone addiction? What kind of insight has that given you?
Beauchamp: So it’s given a lot, for sure. I know that the main antagonist had this relationship with one of the girls in the Good group. I can say the good, but the main group of kids and the reason they’re no longer friends is because he had her do this action for a video and basically got in trouble for the school, but he used that to make this fun video about it. And so she just felt used and taken advantage of. And he doesn’t even remember the video because it was so many videos ago. But the thing I can talk about from the creator aspect in that is that once you get involved in those platforms and if you’re doing it for the wrong reasons if you’re doing it, because what you’re creating is not important. But the following is what’s important. It is endless because you have to keep creating. You have to keep filtering out if you have a weekly or bi weekly schedule. It comes to a point where it doesn’t matter what you put out there, but you have to put something out there or else you fall behind. And that message is pervasive around kids, not just with social media, but work in colleges. I went to speak at a school the other day, and there was a sophomore who came up to me and asked if he had enough research to get into college, like publications. And I was thinking when I was in high school, I wasn’t thinking about research. And he’s like, well, if I don’t do this now, I’ll fall behind. That’s a really common stressor with kids that they’re basically told if you don’t have an internship when you come out of the womb that you’re behind for whatever career you want. And so whether that’s social media, I need to put out this video, and I don’t care about the cost. I don’t care about the people that I affect or how I may have them viewed. Life is moving so fast. It’s this river stream, and if I don’t keep swimming in it, then I’ll fall behind in the game forever. And that’s definitely something I got to attack at in the book from multiple platforms.
Bassi: Interesting. Yeah. I was hypothesizing that in order to diagnose Internet addiction or phone addiction, because it is so ubiquitous to use them all the time. You can’t just look at compulsive use despite harm, because you try to punish a kid by taking their phone away. Well, they can’t do their homework, they can’t watch their classes, they can’t call you to pick them up. You’re taking away this lifeline that they need to function in life. And I feel like almost to make the diagnosis more accurately, you have to think about the purpose, their goals, what is the intention behind that use if it’s just gaming and consuming information or are they learning and growing? But like you mentioned, astutely even if it was learning and growing, you can have these expectations that are artificially placed based on some sort of construct, based on algorithm that are almost impossible to meet when you have other demands going on in school. And in that case, I think I have to go back and think about my theory a little bit better still, fleshing it out.
Beauchamp: Well, it’s interesting you said that about the screen use because I started this research project, it’s going on for the next year here in Savannah, Georgia, where we are looking at kids either with type two diabetes or at risk due to their family life. And we’re kind of taking them through some nutritional and exercise programs over the course of the next year. And when we. Were forming the study. It just got funded and we’re going forward. But we were coming up with, well, how do we measure their success? Do we do it by active minutes? Calories burn, body fat? And even if we do that, what physical thing do we do? And so we were like, oh, we’ll get them all. Like, maybe we can get funded to get them all iPads or something that we can use to track so they can put in their stuff. And when we started talking to pediatricians all across the area, because we’re going to recruit from their offices, they’re like, no matter the socioeconomic status of the family, there is no way in a post pandemic society that these kids do not have a screen of some kind.
Bassi: Yes, totally.
Beauchamp: I hadn’t thought about that. I hadn’t thought about that. Families would save to get their kids and iPad in lieu of other things because of how dark the times were during the pandemic. They want to do whatever they could bring a smile to the kids face. But now we’re past that. You are left. Now we’re transitioning back to society. All right, kids, let’s get back off the screens and get back out there. But for the last year or so, in fundamentally pivotal moments of their psychiatric development, they learned to cope this way. So what do you do as a parent? What do you do as a provider to where this is their normal now?
Bassi: 100%. Guilty as charged. When you mentioned parents can too easily default to just giving them a screen because it’s the easy answer. I 150% agree with you on that. I have a 16 month old, and his first name that he knew was Alexa, because the little pod is in our kitchen and we play children’s music and change the channel and whatnot as he’s eating dinner. So he gets to understand her and how that works. And he sees us on our phones. He knows the importance of them, that they’re valuable and that adults are paying attention to them. And it’s almost impossible to exclude yourself. Like, I’m in tech, I have a job, and any working adult is going to be on their phone. Like, imagine if you couldn’t use your phone whatsoever when you got home from school until the next morning when you left for school. It’s impossible. So your kid is going to see you using them and know that it’s important and then see stuff that’s on TV. Maybe you’ll do it once and slip, or they’ll see their cousins or something with the TV and then they’ll be in a better mood, perhaps. And you’re like, I want to just replicate that. This person is crying in front of me. I got to just fix the problem. Maybe you’re flying and that’s how the ball starts rolling for this vicious cycle. It is really hard.
Beauchamp: I’m not like, faulting or judging the masses of parents that use that as an answer because you weren’t prepared to parent during a worldwide pandemic. And even if there’s not a pandemic, parenting is hard, and you’re looking for anything you can do to make it easier.
Bassi: Yeah, we’re just trying to survive here. We’re tired. We’re hungry.
Beauchamp: I don’t even know what the real issue is. I think the issue is just with the social norm that we’re at now. But the question is definitely where do we go forward with it? Do we need to have, like, a fundamental shift in parenting? Do we need to have regulations and tech use and kids? I don’t know. I’m just throwing questions out there. I certainly don’t know the solution.
Bassi: Yeah, when I worked in the Child and Adolescent Clinic, it was basically our suggestion was putting on controls after hours, limiting the amount on either your router or the settings on your phone itself to turn it off at a particular time. But kids are very smart these days and find ways around pretty much everything, and they know how much you think that you know about them, and so they’re always one step ahead of you.
Beauchamp: So I got asked when I first published, like, what’s the age range for my book? My parents were asking that because with any children’s, young adult book, you need to be very clear on what content there is. And I thought for a second, it’s obviously about a high school student, and there are some, for sure, darker themes. I mean, there’s minor cursing, but what’s typical for kids in what age these days? Because from my experience with kids, they are many adults. They are tiny, tiny adults for what they have normalized to experience, at least in media. And I told people, if you are late middle school or higher, then you should be fine. And I’ve had families, like, who, like, their 8th or 9th grader read it, and then they gave it to their fourth grader, third grader. And then my first thought was, oh, gosh, oh, gosh, the parent note. And the mom was like, oh, my gosh, they loved it. They were talking about this and that, and I was like, I don’t know if I would have read that in the third or fourth grade. Is that what’s normal now?
Bassi: One experience I had with my son actually made me think of your book in a way, and how we have this theme going on here of what is reality and is our reality only simply impacted by our perception? And what if our perception is distorted? Doesn’t necessarily change reality itself, but it’s just our experience that we’re having that’s changing. And my son, when he was first eating different foods other than breast milk and whatnot, he was repulsed by literally everything. Even the most innocuous, bland tasting foods, bread, egg whites, you name it. Like the most simple stuff. He was just repulsed by it. He would make this sour face for anything, really. And it’s like, is that kind of our default as humans, to be grossed out by everything? And we’re taught kind of as an added layer in our frontal lobe, in our prefrontal cortex, to have this, like, top down inhibition of mostly things that are repulsive to us and then learn to like them, actually. So the things that we like are they stuff that we’re liking because there was a learned behavior, because our parents at one point told us that this is important to eat eggs and eat bread and you’ll like it. We eat it ourselves. You should like it. But it’s not like something inherently that he actually likes. He was initially repulsed by it. Right. And it’s just fascinating to think about what about our day to day experiences are actually learned? Like anything, really. There’s millions of different experiences you could think of throughout the day. Is that something that we were inherently driven by, towards, or was that something that we learned based on our societal norms and what we have kind of absorbed through culture to actually value after the fact as this kind of layer on top of our natural desires?
Beauchamp: It’s an excellent question. I think that’s also to just bring that back to the state of med school. I think a lot of the decisions that are made on what we’ve talked about with how students go through their own mental health struggles or go through medical struggles and being vulnerable and open about that, I think a lot of the reason why it’s often discouraged is because it was for them. And maybe when they went into med school, they would have been open about it, but because their preceptors and their higher levels, those cycles just continue. And so it’d be interesting if you could just restart the world and take out the history and plump everybody back into their same positions with no preconceived notions what kind of decisions we’d make for sure. Because I think it would be I think you’re right. I think we do often too much based on what’s always been done versus what feels good and what feels right to us.
Bassi: I love how you pulled that together. That is really 100% accurate, very insightful. That is often just the status quo for a lot of the things that we do, especially in medicine.
New future treatments in child & adolescent psych
Bassi: To round out the theme of the podcast about future psychiatry, is there anything within the field of pediatrics or child and adolescent psychiatry that excites you in terms of new novel treatments?
Beauchamp: There’s a lot. I’m definitely going to hype up a fellow colleague of mine who’s for sure going into child and adolescent psych, I think he wants to do the triple board process. But he just recently finished up this study, which is a full blend of creativity in medicine, which is why I was very intrigued about it. And it deals with kids in psych, but he’s a visual artist and a cartoonist and something he noticed on his rotations and then also with fourth year work with kids is for ACEs (adverse childhood experiences) and specifically for sexual ACEs. The questionnaires that are commonly used for kids, one, are either too clinical to the fact where I think questions can be misunderstood by the patients, or they’re so direct that kids that do understand the question will maybe feel inclined to put a different answer, if that makes any sense. Like, if you have a kid that went through an adverse experience with, let’s say, a family member and a very unfortunate sexual experience, and then you just directly ask, on a scale of one to ten for traumatizing, how traumatizing do you feel that this would like, how is a kid supposed to answer that? And is that the proper way of asking those kind of questions? But that’s how we assess those scores because we need standardization. So what he decided to do was he cartoon and doodled out this whole storyboard of different scenarios. And they’re soft in their imaging. The cartooning is soft, but the images themselves can be graphic because they have to go through very graphic scenarios. And basically, instead of asking all those questions, the kids he had kids go through and pick out just the images that related to them so they would scan through, and there’s an image they didn’t like or like, drew back to that was noted as well. But one, they compared the results of that to the same group of kids that went through the standardization. And with that compared to, like, post analysis and follow up appointments where kids would change their stories and everything and getting a full accurate representation of their experiences, his images were not only I think it was like 60% less traumatic, but they were like 90% more accurate because kids could more identify. I don’t know what you’re asking me that question, but that picture, like, that thing happened to me. And so seeing that he wants to move forward with that going working with neurology and brain scanning to identify what’s the– we say obviously we hate doing anything to our patients that causes them pain, but to find out what the problem is, we cause temporary pain for long term gain. You’ll tell me where it hurts. Does it hurt when I do this? And you especially hate doing those kids, but you’d rather cause them a little pain now and solve their problem. So he’s identifying what is the therapy method with this ACE’s scoring and the cartooning system that can be modified to cause the least amount of trauma, to go through the experience in recounting while still maintaining to be the most accurate in terms of what do we do next. And so he’s working with neurology, moving forward with that. And I’ve seen a lot of stuff like that where they’re using that’s a very creative outlet. He’s an illustrator, and he’s using his illustrations to attack that problem. And when I look across, I see a lot of things in Peds or I feel like a lot of creative people within medicine are naturally drawn because you’re working with the mind, with psych, and it’s in your creative field or with kids who are inherently innocent and see the world creatively. I’m seeing a lot of avenues that combine creativity and research that way that make me really excited to see what comes next.
Bassi: That’s so cool. It makes a lot of sense. It’s almost one of those things that you wonder, why aren’t we doing it that way to begin with? Because they’re calibrated differently with different goal posts at the end of their ten and their zero. And as a clinician, you have different metrics for how you kind of see trauma as well. So to use an illustration or cartoon that it just allows you to map better to their experience. What’s your colleague’s name so you can give them a shout out to them and put it in the resources?
Beauchamp: Dae Gun Kim. Dae Gun Kim. And it goes back to what we were saying before. It’s just the way that it’s always been done. It’s been done by standard for so long. To make any change to the status flow is hard in any field, but I think especially in medicine, with the added hoops you have to go through, because everything you do has to go through some kind of human rights panel and human standardization. It’s a lot harder, I think, than other industries that don’t have to think about those things. So when we make changes to our system, they just take a lot longer, which de incentivizes people to even make changes in the first place.
Perspective changes on the book
Bassi: So cool. Yeah, that’s so true. One thing I want to ask was my experience in making videos. I look back at some of the old ones and I’m thinking of what my mindset was like back then. And you mentioned this earlier when we talked about how you did it. You wrote it two years ago, and your mindset kind of like moved on, but people kind of keep bringing you back to that. And I just kind of want your take on this because the book can kind of be like a time capsule to how you were back in 2020 in the the pandemic, or do you feel like it kind of is going to take on a different perspective? Are you going to look look at it with a totally different perspective, your perspective of 2023 Tyler, the 2023 Tyler who’s now rereading the book. Like, I don’t know if you’ve read reread any chapters recently, but do they come off differently to you now? When do you go back and reread them?
Beauchamp: That’s a really great question. It’s funny. I am the son of a mathematician and my mom, but my dad’s the creative. So that’s where the science and the creativity kind of comes from. Those two kind of raised me that way. But he always said something that really I hold true, that a creative is never really done with any project. They just walk away at some point. And I can’t tell you how many things I’ve written, where I look back and go, what was I thinking? I go back in some of the first stories I ever wrote and me now in 2022 Tyler, I read that and go, that’s bad. That’s just not good. And I remember when I finished the book the first time before editing, I was like, this is perfect. And then the editor did red lines to everything. It’s like, okay, so I’m learning, and I’m so happy with the final product, but I had this fear when I turned it into publishing, and this is it. No more changes. And you sign all that stuff, and every time you sign in the checkmark, this is the final copy, you have to ask yourself again, like, is this really it?
Bassi: No typos, nothing.
Beauchamp: And then you have to wait months before the formatting is in with the sites and you actually get the copy and everything. So I think I didn’t sleep much for those months getting it back, because all I could think about was, oh, I should have done this differently. I should have added this scene. Oh, that character wasn’t fleshed out enough. And I get it now. And you definitely are corroborated a little bit when people say they like the story, which is great. There are a few times I’ve read some stuff at events in the past few months, and even as I’m reading it, I go, I could have used a different detail here. And that’s a good thing for me, because that’s what I enjoy about the process. I really enjoy the writing process. And just like the little tweaks you can make to make something sound more clear and elicit some different emotion. So that’s fun to me. It’s definitely going to be a time capsule, because already the stuff that I’m writing now is just wildly different than that in terms of not just the story, but, like, the the phrasing. I’ve learned I’ve learned so much from the process, having to edit a full book manuscript, you know, 10-12 times I had to go through that story and make 10-12 rounds of major changes. And moving forward, I learned a lot from it. I’m taken away, but I’m definitely a different writer now. But I’ll always be grateful to this story, not just because it’s my first book, but like I said, it was never intended to be published. At the beginning, it was an outlet. It most literally saved me during the pandemic. I went from dreading every day of living in this windowless room and studying and not being able to see family and friends to, oh, if I work and get this done faster or not faster, if I can be more less distracted and taken the information better, then I’ll have more time to work on this after. And it feeded me. It gave me energy that way. And I know it’s a long answer to your question, but that’s kind of what I was trying to explain to people in medicine is that when I was doing that music video, when I was writing this book, or actually when I was doing the best academically in medicine, not the worst, it didn’t detract. It pushed me to be better in that because the work I did in medicine feeded my creative work and my creative work feeded my energy in medicine, and they just add to each other, which is never a question of taking time away from one or the other. They’re a necessity to me.
Bassi: Yeah, I 100% agree. And it reminds me of this quote, if you want something done, ask somebody who’s very busy.
Beauchamp: I love that.
Bassi: And I love your dad’s quote, too. I’m going to have to use that and provide attribution to him, of course, Mr. Beauchamp. But I think I’m going to be saying that in the future because that reminds me of step one and step two and all the board exams. You’re never ready. You just have to keep going and say, all right, I’m going to take this exam. Even though you never feel ready for it, you’re probably like, I can go over that chapter again, and I can go over that chapter again. If you never had that deadline, I’m sure people will just push it off, push it off, push it off. But it’s so cool because to hear your experience in the writing process itself, I really appreciate you talking about all that. So cool.
Beauchamp: Thanks so much for having me. I really enjoyed coming on and talking about just not just the writing, but the medicine and hearing from someone who lives a day in, day out. But you’re also doing it too. You’re being creative while keeping the medicine going. So I can’t tell you how much hope and ease that gives my mind when I see someone in the field doing that, because I very much want to keep this going. And sometimes I wonder, is it possible to do it long term? But when I see people like you doing it, it definitely makes me feel like there’s hope.
Bassi: Yes, absolutely. I mean, I think you having this experience and hobby and writing and keeping that going will allow you to get through these next few transitions even easier. Because I can kind of relate to this. Every transition is a new stressor on your spirit and your psyche and adjusting to new way of life. But if you have something that’s a constant that you can fall back on, that you feel like provides you meaning and value, I think that makes the rest of your life easier. When you’re going through that transition process, a lot of new attendings, they kind of feel like– because you always have this carrot in front of you to get to the next thing. And for the last eight years, you’re just thinking about the next exam, next vacation coming up, and then when you’re attending, it’s like, all right, I’m here. What do I do now? Is this my life? I’m just doing this 45 hours a week? Yeah, totally. Keep the balance, keep it going. It’s definitely, obviously opened up a lot of doors for you and interesting conversations and new impacts that it’s had on a lot of other people around you. So pretty awesome.
Beauchamp: I appreciate you saying that. Thank you.
Bassi: I’m going to have to interview more authors on the podcast because I really like this conversation and there’s so many parallels to medicine, too.
Beauchamp: I get very nervous on live TV, and I’ve had to do that a few times, and there was one time, though, where I was like, okay, if I can just take this sound clip and then you just use that for the others, then I don’t have to go on live TV again. Just use that one. Someone asked about, like, how is it possible for you to do when one is so left brain and one so right brain, how do you do both medicine and writing? And to me, I think I’ve said something along the lines of, like, it’s not different to have to write something and know, if I don’t write this in a way that it connects to a reader and gets them to feel the way that I need them to feel, then I failed at my job. The same way if when I go into a room and I don’t know somebody, if I can’t connect to them, it doesn’t matter what my treatment strategy is, they won’t do it. If I can’t connect to them on an emotional level and understand their mind and where they’re coming from exactly, then I haven’t done my job. And the same goes true with writing. You can’t just write what you want to write and how you would perceive it. You need to write with your audience in mind and how they perceive it, and then you can combine the two, and you can get the two to come to a common ground. But there’s so much overlap in writing and medicine.
Bassi: That goes back to the contextual errors that I was talking about, and I think medicine is a lot more right brain than people maybe let on at first. Well, Tyler, very much appreciate you being on the show and sharing your insights and really enjoyed the conversation. Really cool. I think a lot of people would benefit from hearing this, so I appreciate it.
Beauchamp: Thanks for having me, it was a blast.
Bassi: As a reminder, if you’d like to support the show, one way you can help us is by subscribing to the channel on YouTube and leave a comment if you’d like. It also means the world to me if you can share it with your social media network, maybe there’s somebody out there who might be interested in the podcast. Hope to see you next week. Next Monday. New episodes are released every Monday morning. Thanks a lot. Take care.
Resources
Tyler Beauchamp’s Website, Link to Purchase Book:
https://www.tyler-beauchamp.com/
Contextualizing Care Organization w/ Dr. Saul Weiner
https://www.contextualizingcare.org/
Contextualizing Care Podcast Episode
https://onbecomingahealer.libsyn.com/contextualizing-care-a-new-study
Dae Gun Kim’s Research Poster on the development of pictoral representations of adverse childhood events

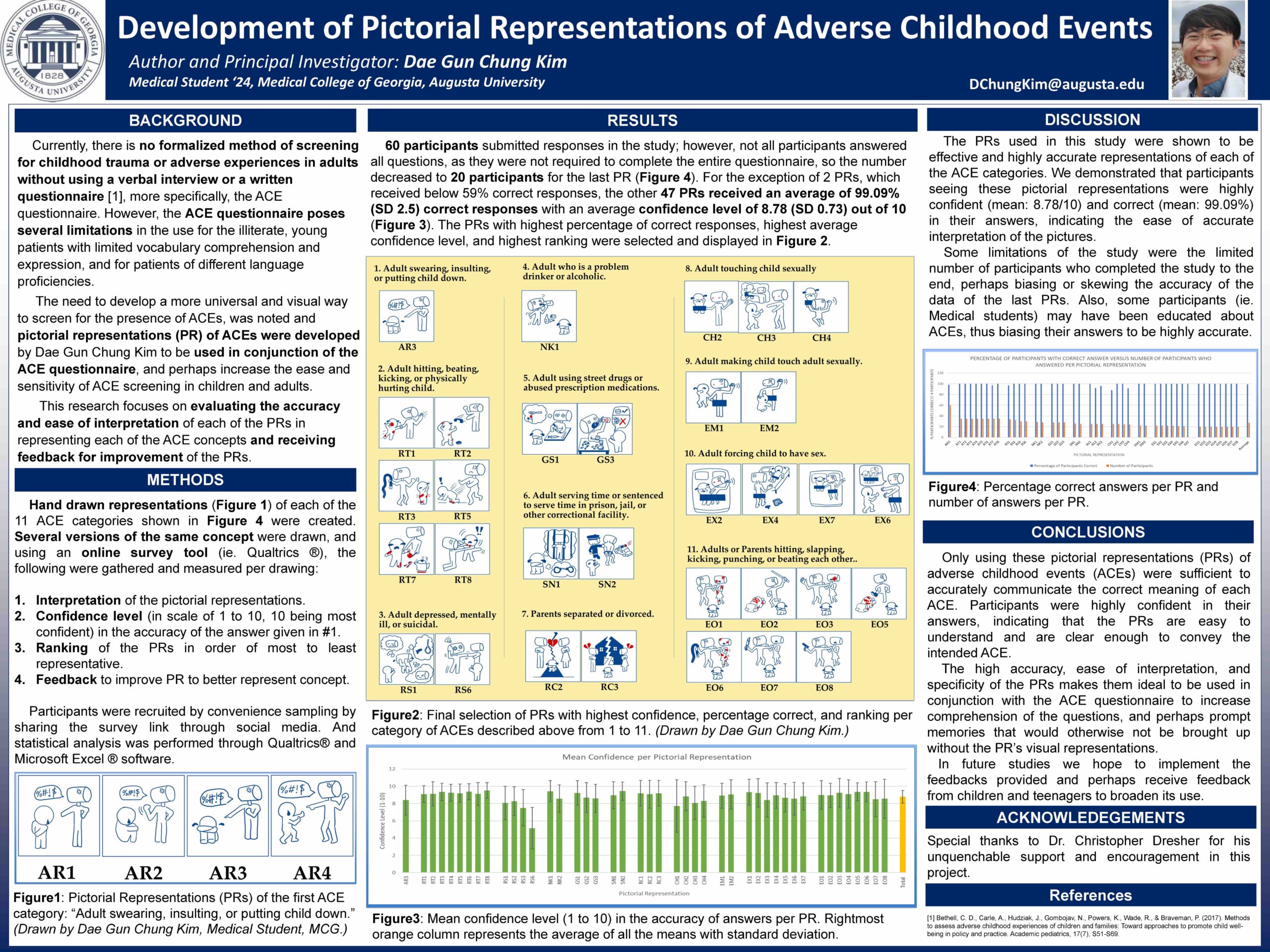{kind=link}